A Discharge Summary Template is a document that summarizes the hospital encounter of a patient and identifies encounters, care processes provided, and progress and discharge instructions. It may contain crucial data like the patient’s identity, admission and discharge dates, diagnosis and prognosis, medication records, treatment regimen, appointment scheduling, and guidance on further care.
The purpose of the Discharge Summary Template is to support and enhance collaboration between different medical professionals to avoid discontinuity of care and guarantee that the patient continues receiving the necessary treatment after he or she leaves the hospital.
A Discharge Summary is an essential document that is given to patients when they are being sent home from the hospital or healthcare institute. This is the basic information transfer medium between the hospital and the primary care providers. This summary may contain some vital information like medical history, diagnosis which led to admission to hospital, treatment given, surgical interventions, etc.
Further, it explains the patient’s condition at discharge, the medications provided, and other aftercare instructions. It is crucial for the care of this patient not to be interrupted and for potential complications or readmission to be avoided.
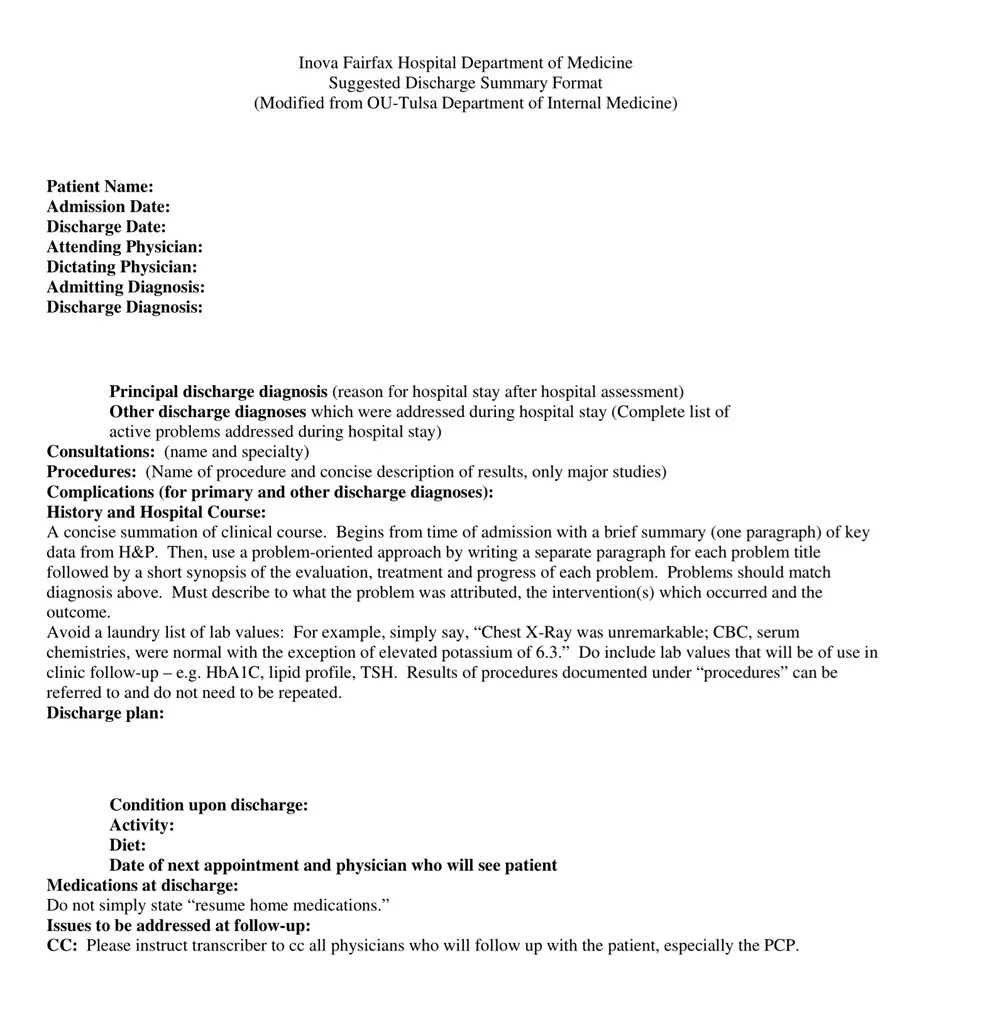
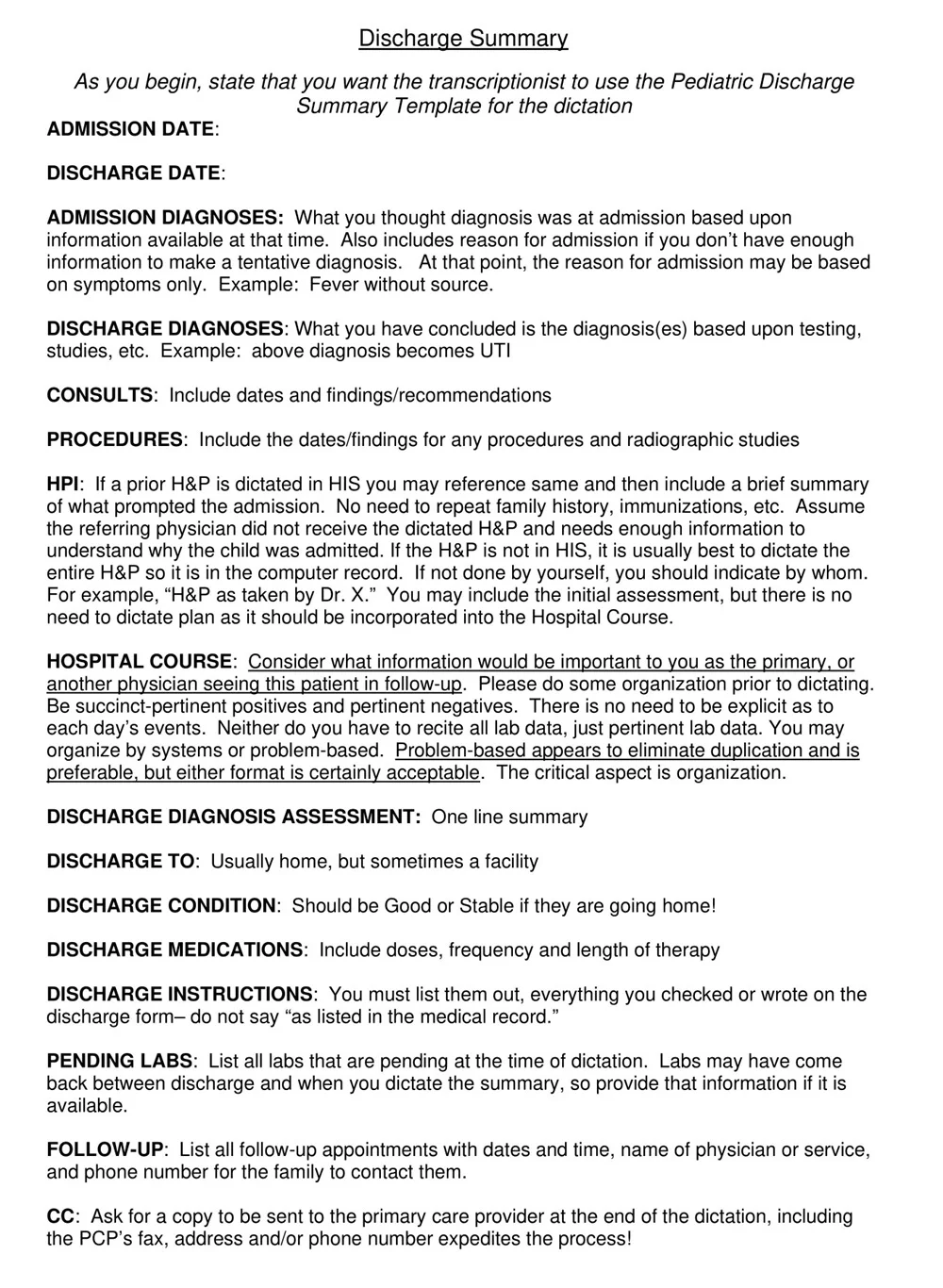
What Should a Discharge Summary Include?
A discharge summary is an important part of the continuum of care as it contains information that is necessary for further treatment of the patient.
It should include the following components:
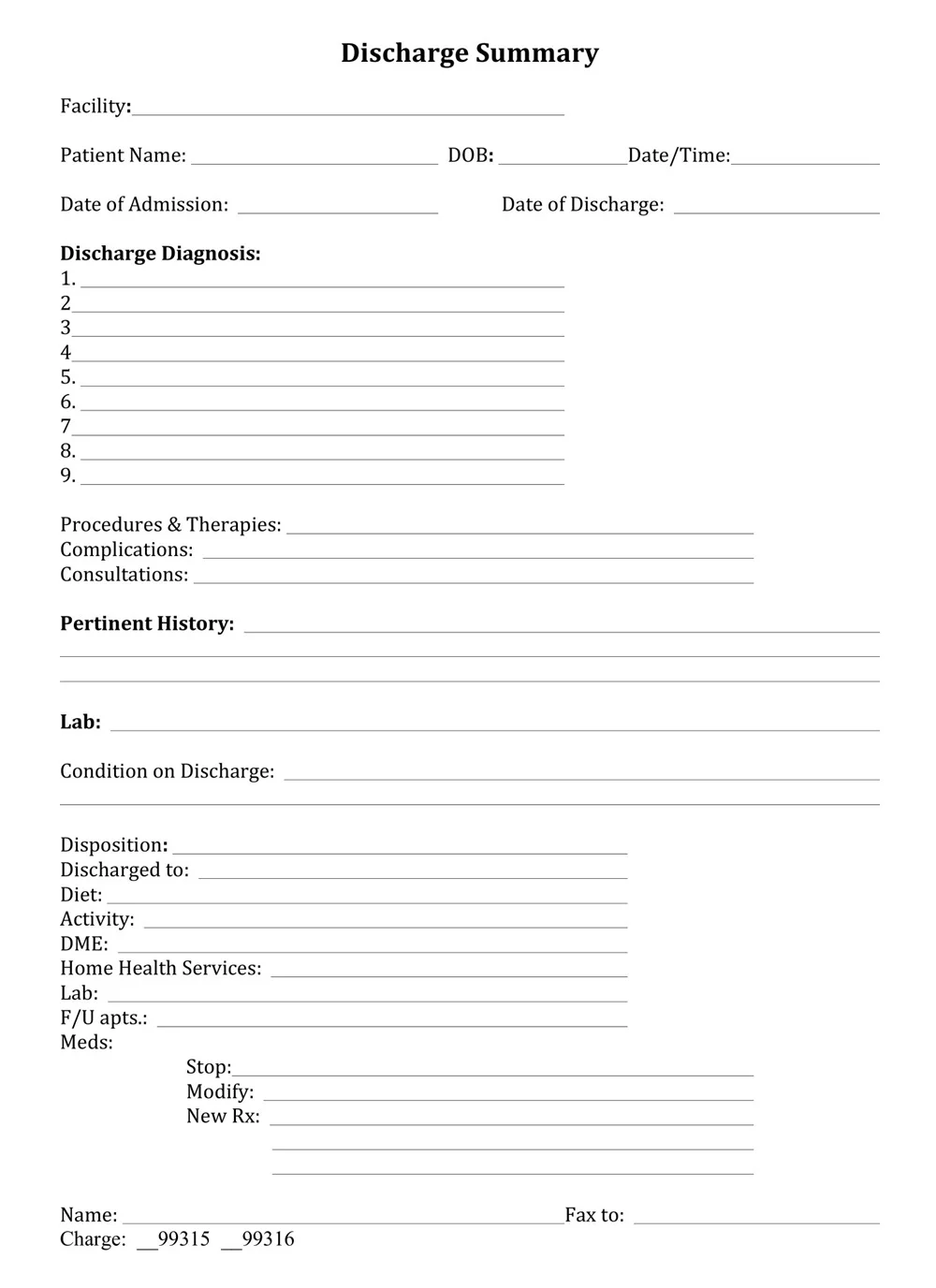
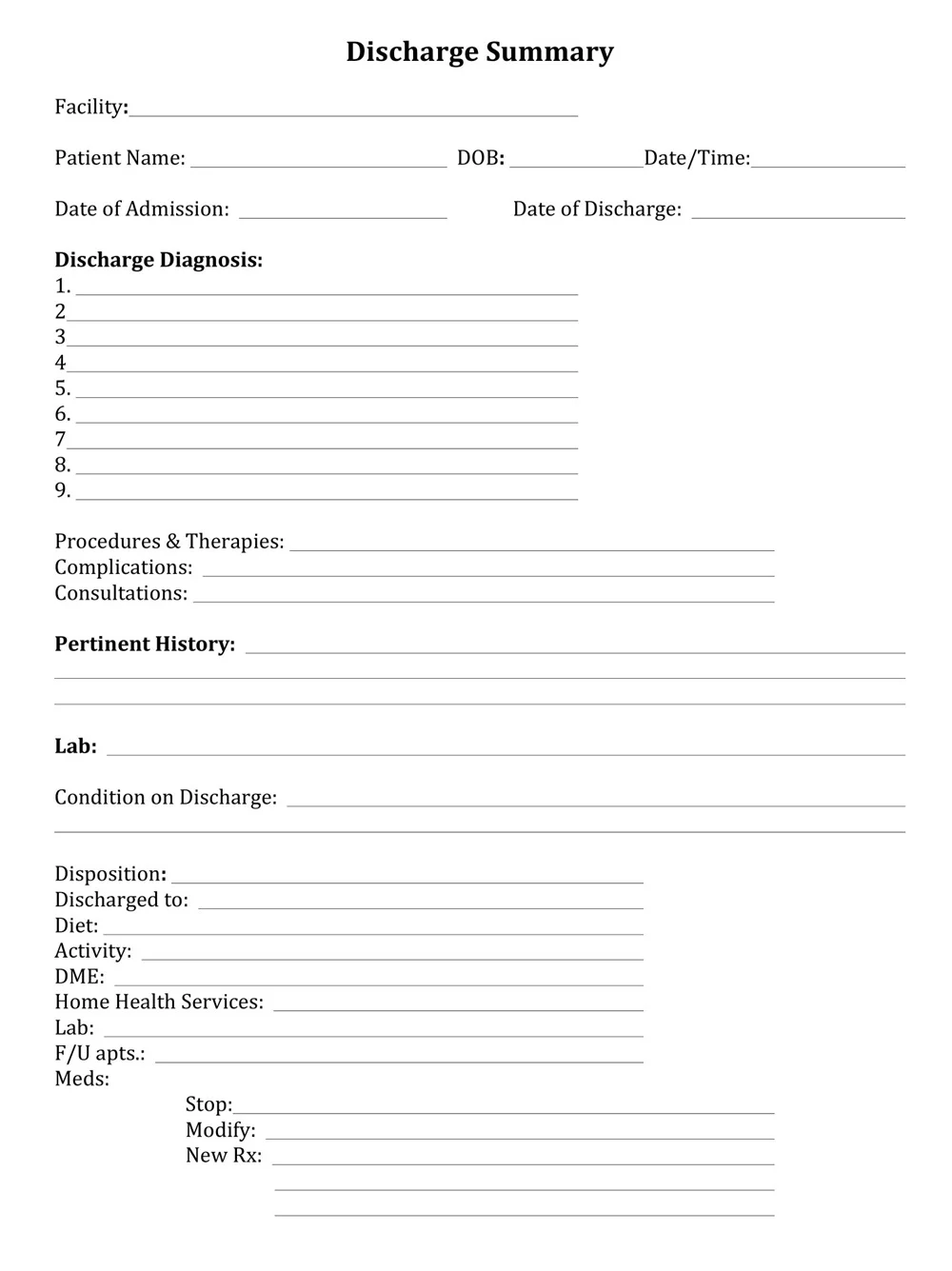
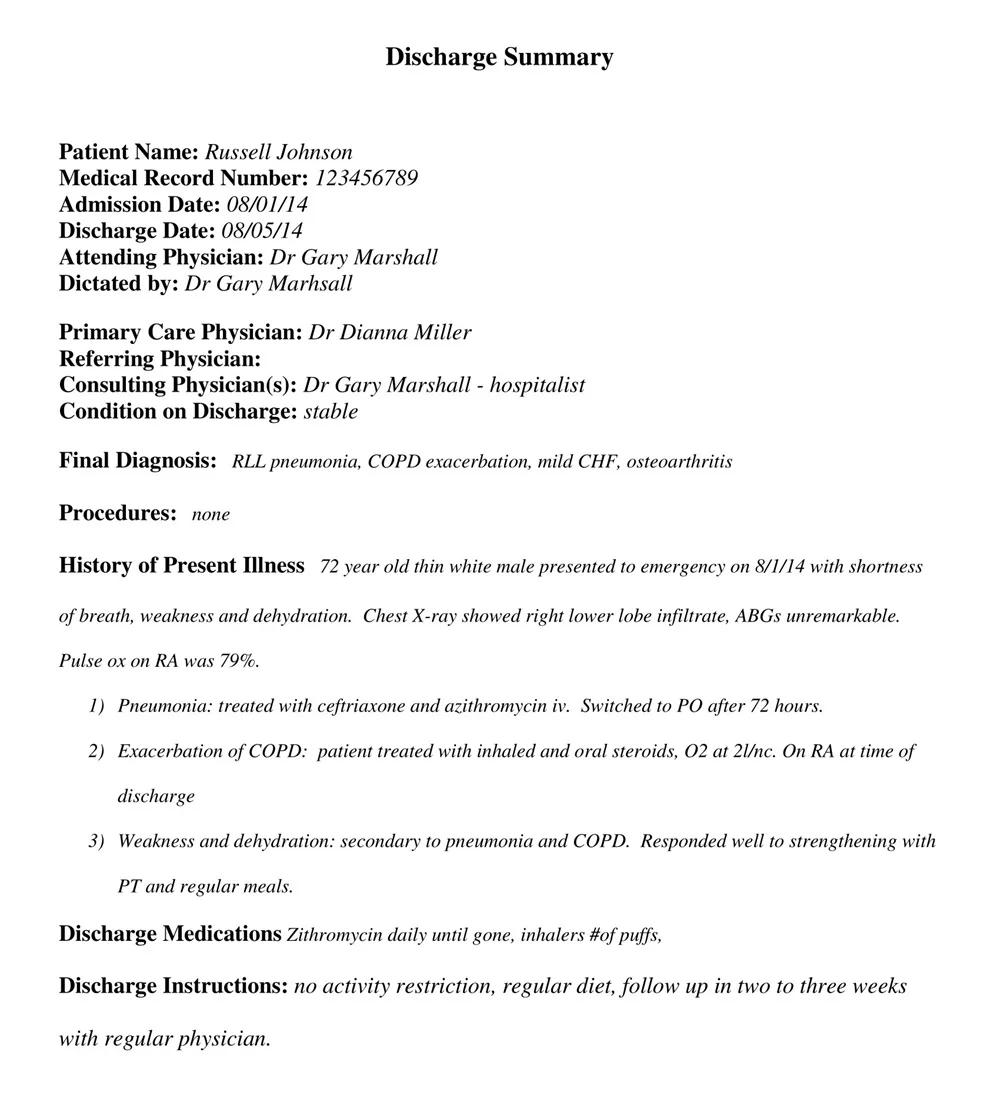
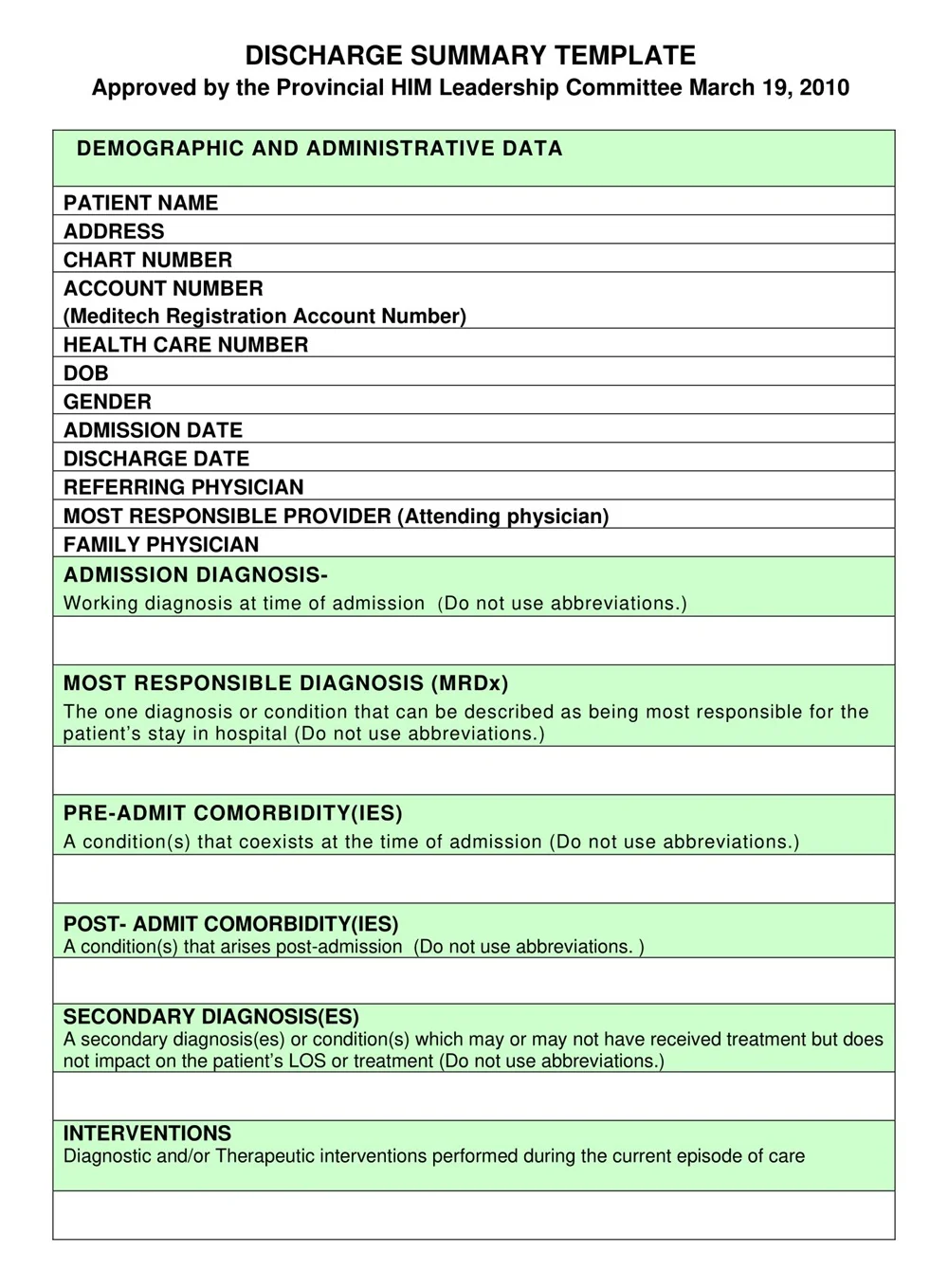
Patient Information: First name, middle initial, last name, date of birth, street address, city, state, zip code, phone number, and medical record number.
Admission and Discharge Dates: The period during which the patient was hospitalized in the hospital.
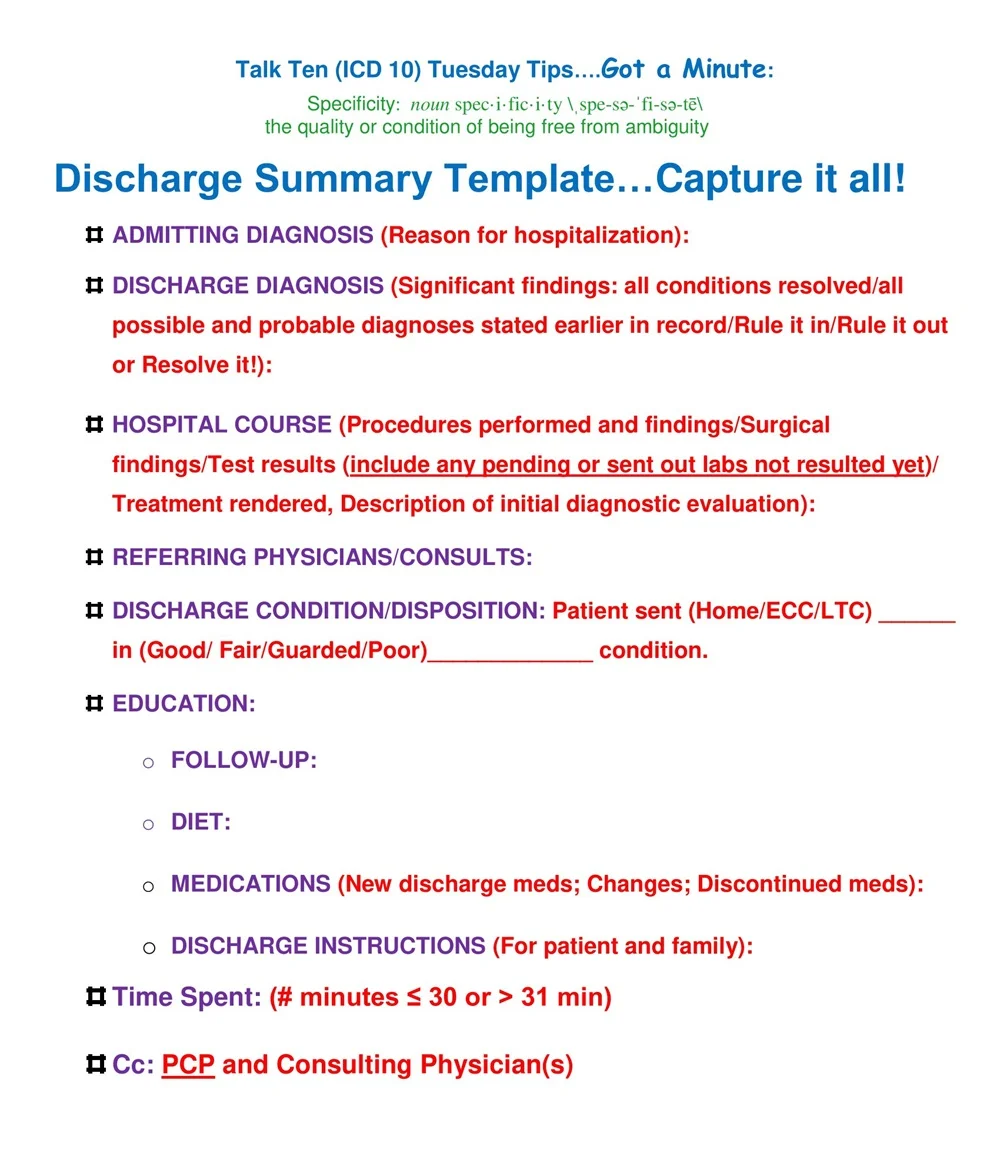
Diagnosis: Data on the principal discharge diagnosis, secondary diagnoses, and potential hospital-acquired conditions.
Treatment Course: A brief outline of treatments given and any medications, operations, or other significant interventions.
Medications: A complete medication list, provided at discharge, with dosage and frequency of administration.
Follow-Up Care: Related advice regarding further appointments, referral to speciality services, and any required follow-up investigations or procedures.
Patient Status: Aspects of physical and mental health at the time of discharge.
Instructions for Care: Specific recommendations for post-hospitalization nutrition, behavior changes, and things to avoid.
Emergency Contact Information: Contacts in the event of an emergency or possible complications.
These elements are included to make sure that the discharge summary is not just a document but can be used by the patient and caregivers as well as the healthcare providers to evaluate continuity of care and readmissions.
Uses of Discharge Summary
A discharge summary is a medical report that includes information about a patient’s admission and subsequent treatment, as well as instructions for follow-up care. This document will be helpful for the transfer of care between providers and for legal purposes. Here one can find some of the key applications of discharge summaries in the medical environment.
Continuity of Care
A discharge summary is a very valuable means of supporting follow-up care. It informs healthcare professionals of the hospital course, treatments tried, and the response to treatments. This helps primary care physicians and other subsequent caregivers to determine the best follow-up care and make appropriate choices.
Communication Tool
The discharge summary is a key link between hospital staff the patient’s primary care physician and other consultants who may have been involved in the patient’s care within the hospital. It helps avoid confusion and ensures that the medical history, the plan of treatment, and any guidance for further care are well understood by all involved.
Legal Documentation
In case of medical disputes or legal inquiries, the discharge summary is the official document depicting the hospital stay and the care details of the patients. It can be used as a legal document that proves that medical standards and protocols were met and thus ensures the security of healthcare providers and patients.
Insurance and Billing
This is especially true when insurance companies demand a lot of documentation for claims to be processed efficiently. A well-written discharge summary also helps in the billing process since it demonstrates evidence that the right kind of medical services have been availed and hence should be compensated.
Patient Education
Last but not least, the discharge summary is a useful tool for patients and their families. It contains vital information like medication guides, follow-up dates, and advice on certain lifestyle changes that patients can use to take care of their health after being discharged.
Importance of a Discharge Summary
A discharge summary is a key component of the patient’s medical transition process. It also fulfils the role of communicating the hospital-based team’s findings to subsequent care providers and thus acts as the measure of transition for the patient from the inpatient to the outpatient department.
A discharge summary is a document that summarizes the information about the Hospital stay of the patient like diagnosis, Treatment given, Progress during the hospital stay, and Complications if any. It also writes post-treatment advice like care instructions, and prescribed medicines, and suggests further treatment. A discharge summary is important for ensuring the quality of care and continuity of care and also preventing readmission to hospital and medical errors.
Benefits of Discharge Summary
A discharge summary is one of the most critical documents that are crucial for summarizing the entire hospitalization process of a patient and their further treatment and recovery. It contributes towards ensuring that the providers of healthcare engage in proper communication with each other and it also ensures that the healthcare received by the patient is continuous. The following part will focus on some of the positive aspects of having a complete discharge summary.
Improved Continuity of Care: The discharge summary plays a critical role in conveying information to the primary care physicians and other allied health professionals; it will make the noting health care provider aware of what has been done in the recent past and whether the patient still requires any form of treatment or intervention.
Enhanced Patient Understanding: Summaries can assist patients and their families in comprehending the healthcare they received, the meaning of follow-up visits, and the instructions about medications, diets, and exercises.
Reduction of Readmissions: By providing specific information about post-discharge treatment and care, the discharge summary document assists in the readmission avoidance process to ensure patients receive the correct care and information.
Effective Communication: They act as a way of communicating essential data about a patient from one healthcare setting to another in a way that is less likely to result in the loss of such information.
Legal Documentation: Discharge summaries can act as essential legal documents for future reference in case someone disagrees with the services offered or seeks to claim the hospital.
Time Efficiency: They facilitate the work of healthcare providers by extracting the main information and saving time that could be used for the patients’ file analysis.
Supporting Health Management: This is reflected in discharge summaries where advice for change in lifestyles and home care are provided to ensure the long-term health and well-being of the patient.
How to Write a Discharge Summary Template
Discharge summary is a cumbersome task but if a template is formulated beforehand then the task can be easier and more time efficient. This article presents the required steps in creating an efficient discharge summary template.
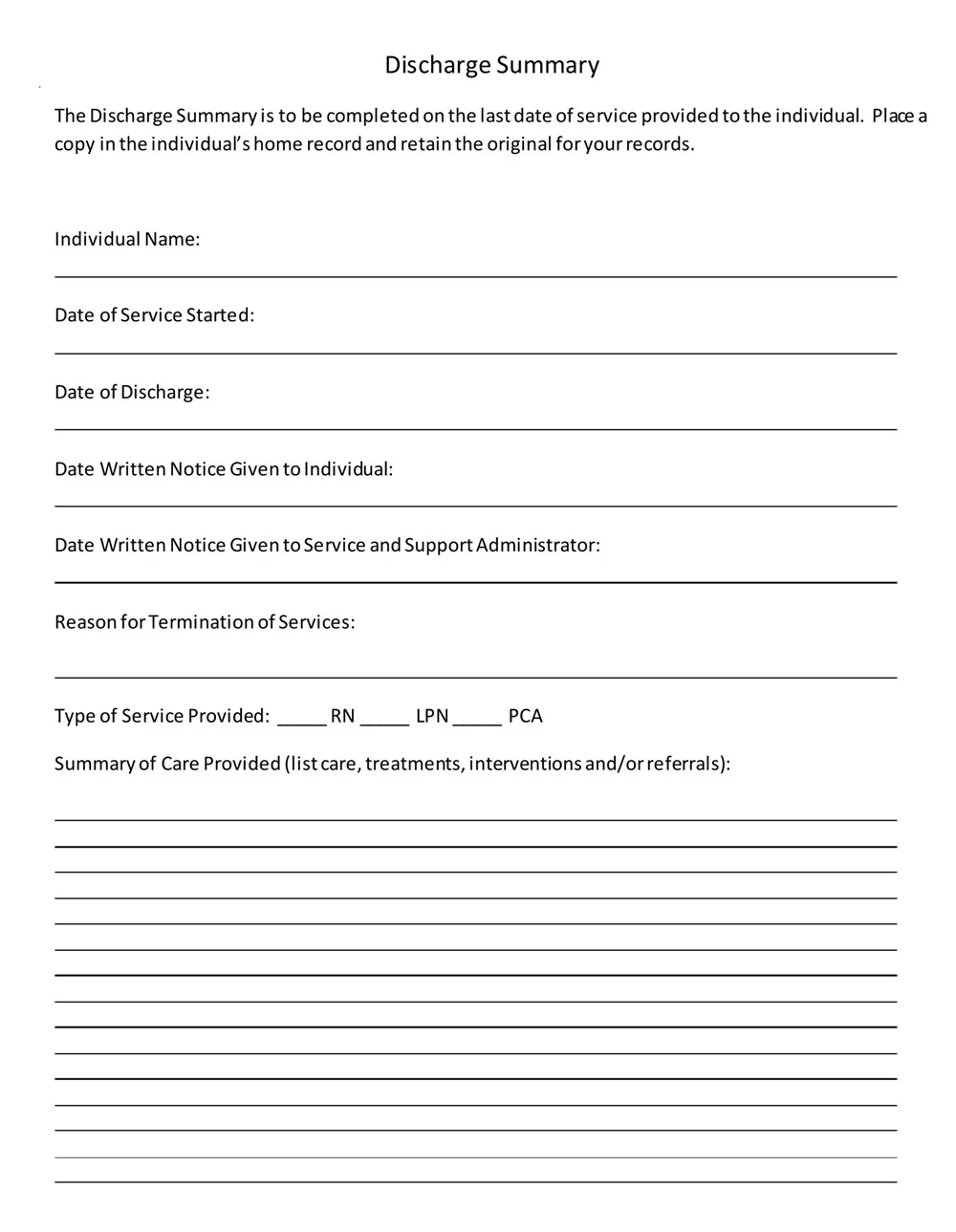
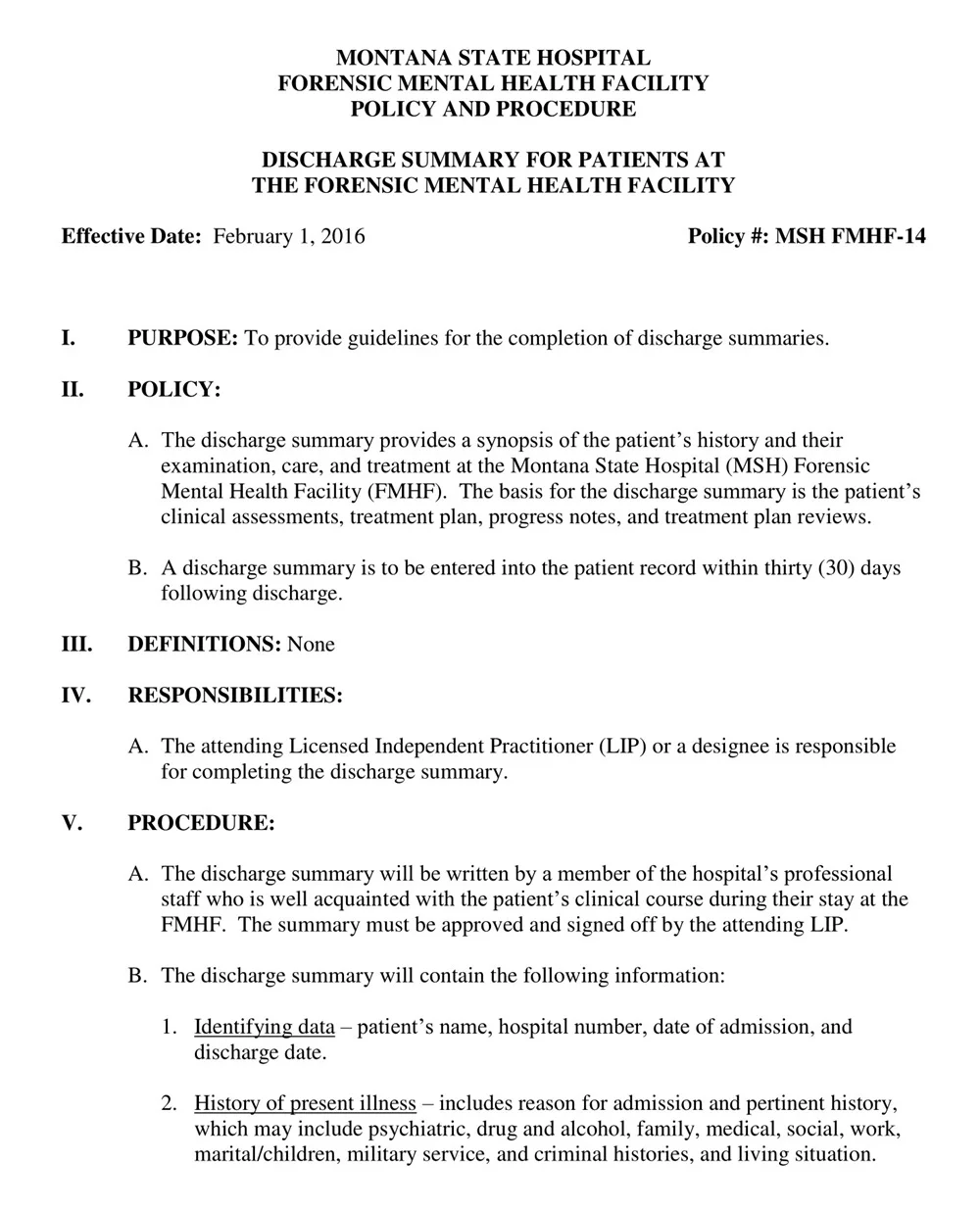
Step 1. Include the Patient’s Information
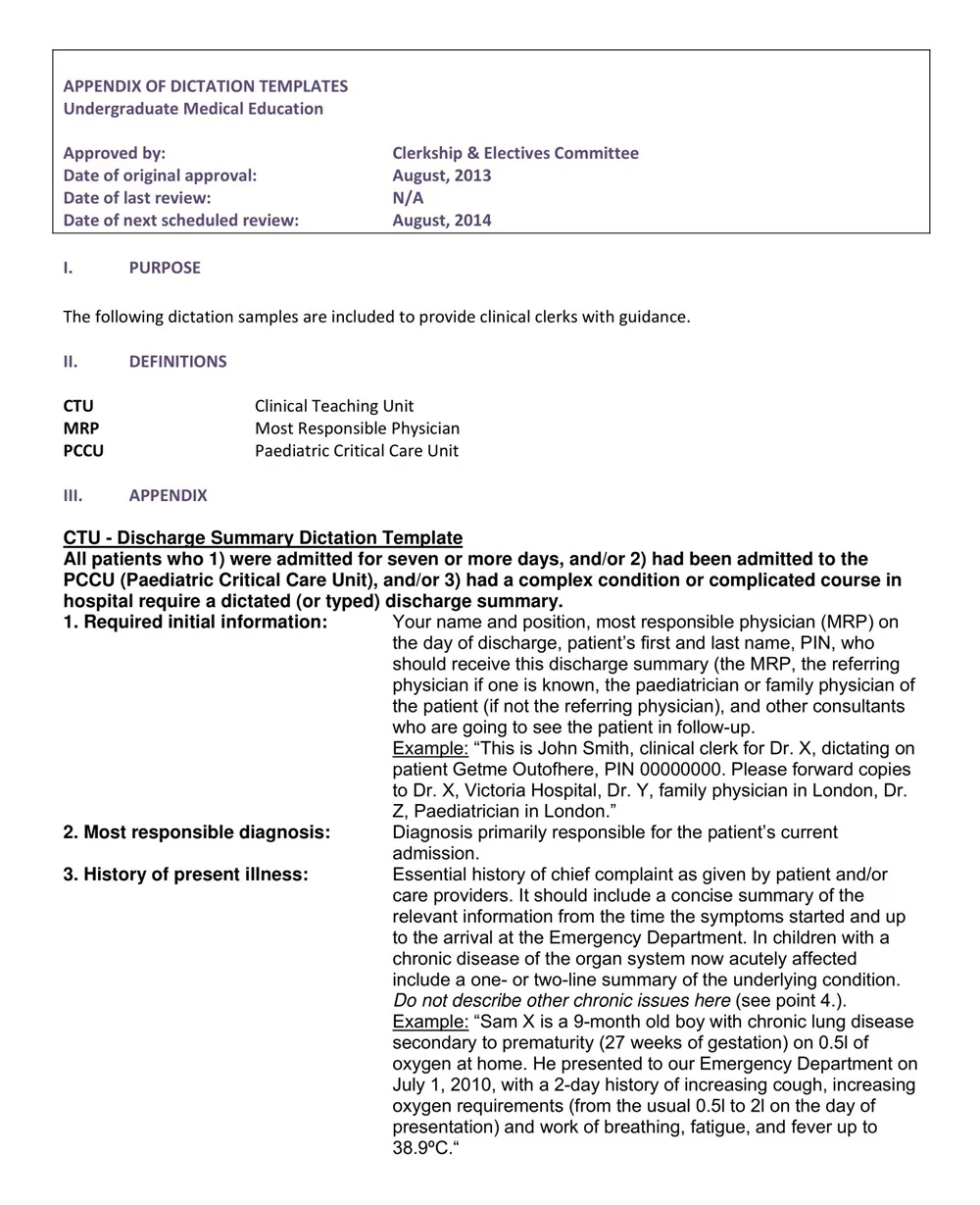
The first part of a discharge summary should consist of some general information about the patient, like the exact name, age, date of admission and discharge to the hospital, past medical history, etc. This helps the clinician to determine whether the right patient is being discussed and also gives the context for the current hospitalization episode.
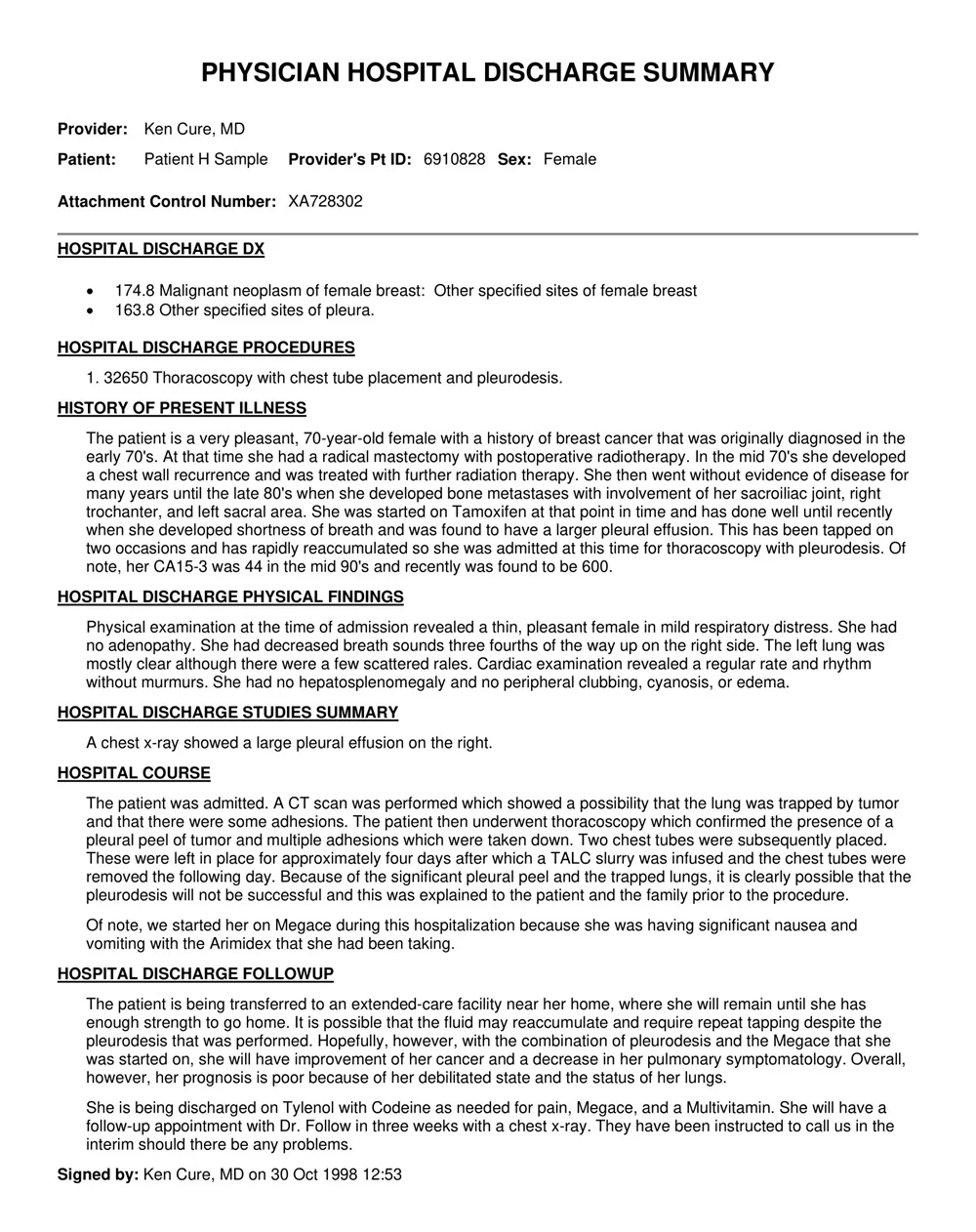
Step 2. Summarize the Reason for Hospitalization
Then, offer a concise history or explanation of why the patient was hospitalized. This may include their initial symptoms, final diagnosis, and any therapies or interventions that were conducted during their hospitalisation.
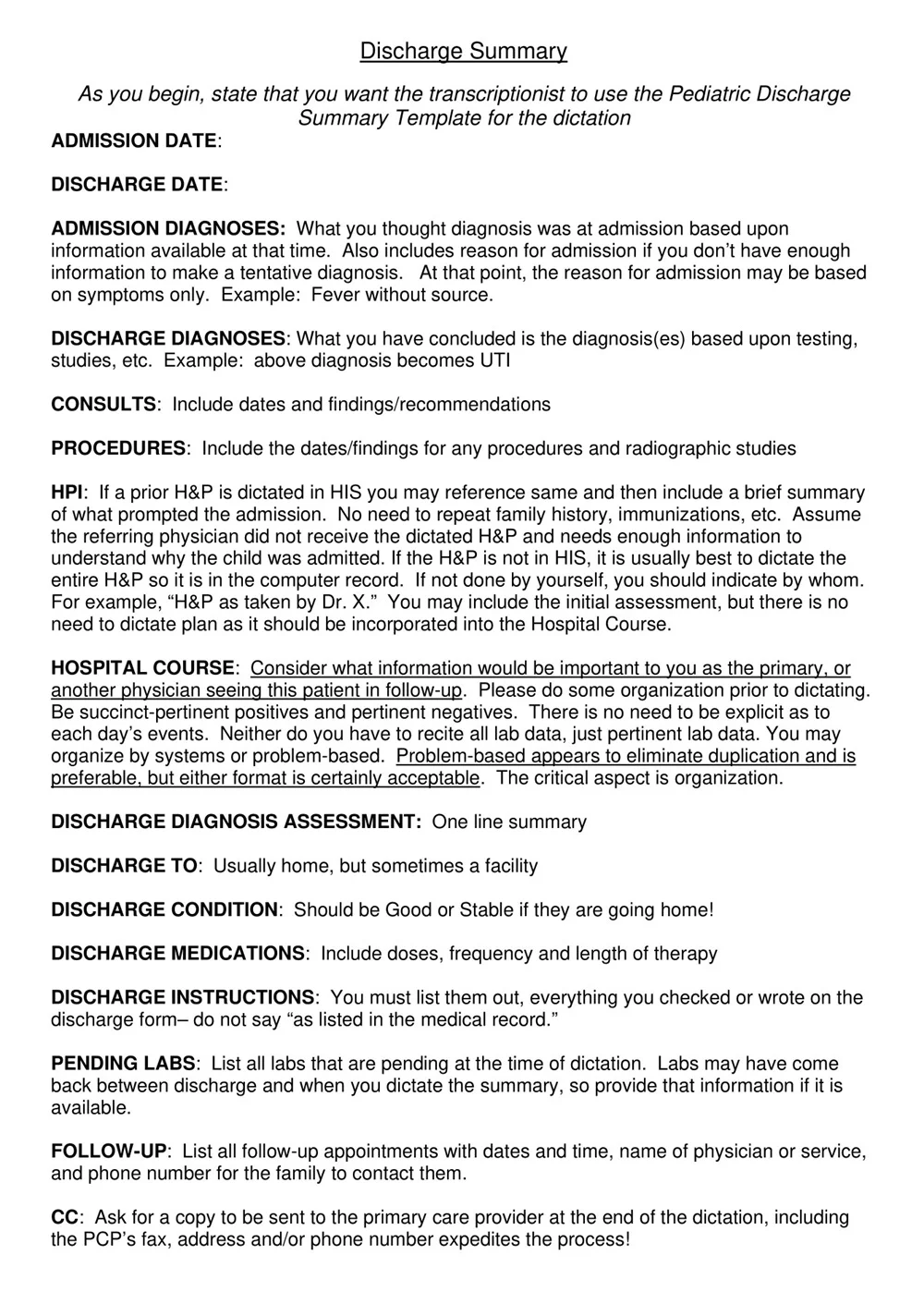
Step 3. List All Medications Prescribed
A particular emphasis should be put on the comprehensive medication list that was provided to the patient during the hospital stay. This includes any amounts that were increased or decreased alongside the new medications introduced during their stay.
Step 4. Document Any Follow-Up Instructions
The discharge summary should also indicate any specific instructions that the patient should stick to after being admitted to a particular hospital. This could be appointments, medication timings or certain lifestyle changes that a person is expected to adhere to.
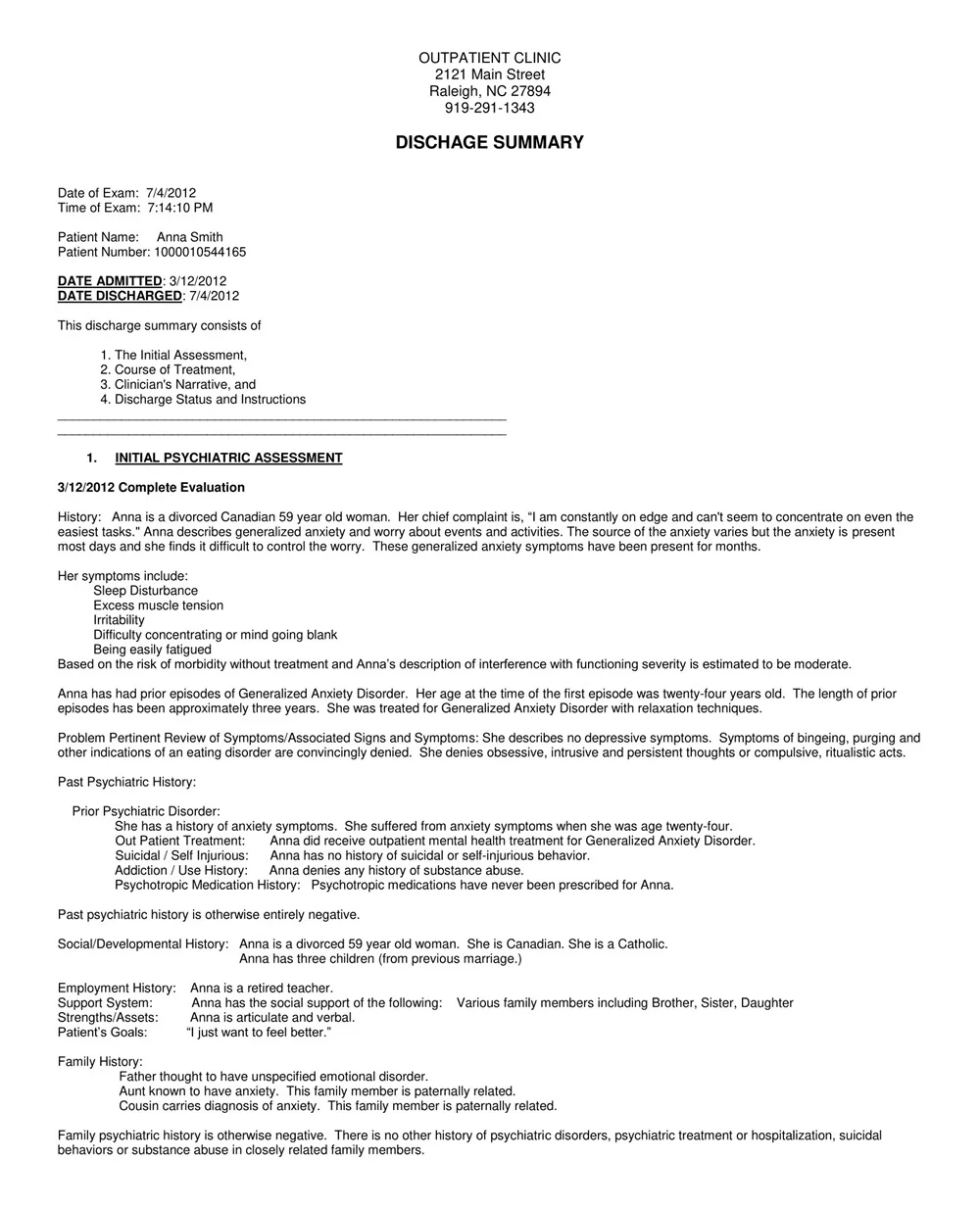
Step 5. Include a Summary of the Patient’s Condition at Discharge
Here report briefly about the patient’s condition at the time of discharge from the hospital. This may be their temperature, their blood pressure, the presence of any symptoms or issues they may be experiencing, and any restrictions they may be subject to.
Step 6. Record Any Advice Regarding Further Treatments or Follow-up
It is also important to document any additional treatment that the patient might need after discharge or follow-up care. This could be, for instance, any of the following: referrals for the patient to see other specialists; reminders for follow-up tests that the patient might need; or a care plan for the patient.
Step 7. Review and Proofread
It is always advisable to recheck the discharge summary template for any omissions or mistakes before filling it. When completing the document, it is necessary to pay attention to the completeness and correctness of all the information and make the text clear and understandable.


")


")
")
")

